
%20copy.png)
.png)
Transcript
Marla: Welcome everyone, and thank you so much for joining. We are talking today about high growth habits and how to fuel practice growth in 2026. I'm Marla Ranieri, I'm the head of clinical innovation and clinical strategy at Prompt and I'll be your moderator for today. Um, we have an incredible group of panelists with us, actually some goats in the industry, so really excited to have them here.
And we're gonna be unpacking behaviors, habits, and systems behind high growth rehab clinics. Uh, we really are doing this 'cause we did a great survey recently. We looked at 600 practices across the us. They were all sizes, all growth stages with all different EMRs. And it was an industry-wide survey. It was not just prompt clinics, all types of clinics.
And we asked some key questions because we know everybody is facing the same reimbursement problems, staffing issues, operational friction. Yet there are some clinics that are growing really well, 10%, 20%, even 30% year over year growth. So we really wanted to know what are they doing differently? What is it that high growth clinics are doing operationally?
What are they doing strategically and what are the gaps between those are do that are growing at that level, super high growth, and also ones that are maybe stagnant or starting to decline. And when we defined what growth was in the survey, we had low growth as less than 10% or declining. Um, or flat. We had high growth as greater than 10%, and then we had super high growth as greater than 20%.
And what we saw was that 83% of clinics are growing year over year. So that's great to see that most clinics are growing, but only 50% are scaling above that 10% and are high growth clinics. So with that, you know, we said everyone's got the same pressures, so what are they doing different? What data are they using?
What systems, what strategy? And that's where we're really excited to have our panelists to talk a little bit about what they see and where they can help and give you guys some insights and practical strategies that you can apply immediately to your, your practices. Um, before we start though, just wanna do a little housekeeping.
We do have the chat open. Feel free to chat with each other. Say hi, who you are. Um, as well as there's a button on the bottom and that's our q and a button. I would definitely hope you guys use that one for any questions, not the chat, because then when we answer questions at the end, we can go from there.
And if we don't get to your question, we will absolutely email you later and make sure to get back to you. So just use that q and a question for any questions that come up throughout the session. Uh, there will be a couple polls along the way and please answer those as well. We want your engagement. We want this to be as much about you guys as it is about hearing from us, and make sure that we we're listening to you as well.
So first poll, just quick pulse check. You're gonna see a popup. And it's gonna say, which best describes your clinic today? Are you struggling to grow? Are you stable but plateaued growing slowly? Or are you in that high growth scaling mode where you are keep growing as well? Alright, everyone take a second to answer that.
Perfect. And now I will introduce our panelists. So as I said, we've really got a great group here for you. Um, first we have Jeremy Van Ner, who is the strategic advisor, consultant and operator for greater than 25 years. He's a founder and managing partner of Equi Growth Advisors and he brings his deep experience, uh, from his executive roles as a former Chief Revenue officer of Ivy Rehab and he's been scaling national outpatient therapy networks and building growth oriented operations for greater than 25 years.
Jeremy is such a pleasure to have you.
Jeremy: Hey, hello. Good to see you again.
Marla: And we also have Ken gdo, who is the co-owner of and CEO of three dimensional physical therapy. Uh, it's a high growth, multi-location practice. So he is actually in that high growth, uh, group that we, that we saw in our survey. Um, he's also a co-founder of IPTA, which is a New Jersey super group.
It's a group that has over 16 companies operating under a shared infrastructure, and he brings a rare blend of clinical excellence, entrepreneur leadership, and having built a multi-location practice grounded in patient experience, sustainable growth. Uh, such a pleasure to have you today, Ken.
Then we also have Josh Grover. He's a co-founder of Optimized Transition Partners, which is a business coaching company that helps clean up billing and brings it in-house, as well as the Director of client success and coaching at Prompt Health. And he is a former COO of Spine and Sport, uh, in New Hampshire.
And he is got deep experience in revenue cycle, financial discipline, and unlocking operational performance and outpatient practices. Uh, he really brings a special bridge between clinical excellence, business health, and cash flow strategies. Thanks so much for coming, Josh.
Josh: Thanks for having me.
Marla: Great. And just to start and frame this out, I'd love to hear from all of you in a few words, what is one high growth area that clinics.
That are high growth, execute well, um, and that plateaued clinics tend to overlook. So, um, we'll start with you Ken. What do you feel is one area that high growth clinics execute? Well
Ken: first, can you hear me now or are we good? I can now. All right. We did it. Yeah. All right. So, um, basically, so with that super group and with that IPTA that, that Marla was speaking of, I've had the opportunity to talk to a whole bunch of different practices.
Um, the biggest thing that I've seen is, is the owner understanding their role as an owner in growth. Um, so you need a why a mission. You need, uh, consistent and clear communication. You need to develop that culture and environment that people actually want to come in for therapy and people actually want to come in and work.
Um, you need to remove barriers, obstacles for your team. Then you need to be a clinician. Like I think some owners, uh, uh, maybe kind of lose sight of their role in growth.
Marla: Perfect, perfect people culture, mission. I love that. Um, and Josh, what about you? What is one area that, uh, high growth clinics do really well and less maybe overlook?
Josh: I would mirror Ken there. I think it trickles down even to the, the, your clinic directors, right? Um, switching from the PT mindset to an actual clinic director and what they need to be overlooking, how they need to start thinking about your operations, the, the volume and those types of things. I think another thing that high growth does really well is they have playbooks to turn the important things into valuable things.
And what I mean by that is there are a lot of important things that need to be done, but they can be automated. And some of those people that are doing those important tedious things that can now be automated, they're actually going out and being proactive and doing things that are now valuable as opposed to just important.
Um, I think a lot of high growth, uh, is able to do that. Um, I don't wanna say run lean, but maybe run more efficient, uh, by, by doing those things. Okay.
Marla: Great. Great, thank you. And Jeremy, what about you? What do you feel is an area or a pillar that high growth clinics would do really well in?
Jeremy: Hard to go last, because the first two ideas were the things I would've said as well.
So mirroring what, uh, Ken and Josh said, absolutely. I mean, culture is the centerpiece here. Um, it, it's all about a, a culture of accountability, teamwork. And at the end of the day, it's putting the patient in the middle of that. Uh, I think sometimes we get really lost in there's metrics. There's financial, there's, you know, all the work that needs to be done.
But at the end of the day, you're only as good as the engagements with your worst, with your worst patient, honestly. Um, every patient that comes through your door is an ambassador. Uh, every patient you see is an opportunity. And what I've often found is that we get lost in the mire of my, you know, looking at financials and complicated stuff and all that stuff really matters.
But at the end of the day, every patient that comes through your hands is gold. And if you lose one, that might cost you 20. Uh, and I think we lose that, that track of that quite a bit. One of the thing I would say, uh, beyond the culture is just there's a, uh, uh, there's an intentionality. Um, and there's a dedication across all teams.
You, you can't be successful in scaling a business if you're a team of one. Um, I've experienced this in consulting experience this as a clinic director and, and, you know, being an executive in an organization, it's truly intentionality and it's starting conversations with why, why does it matter to grow?
Well, in, in my view, it's all about the opportunity to expand your brand, expand your presence, um, you know, build those connection points with patients. And if you have that level of intentionality across your entire team from the part-time staff that's helping you out to all of your therapists, that to me is the recipe for success.
And it also builds a bench and a capability to not have it be all about one person. You, you just can't thrive and grow successfully when you're curing the weight of the world on your shoulders.
Marla: Perfect. Perfect. And I, I'm really hearing from the three of you, it aligns with what we saw in our survey. Um, we saw there was three pillars of high growth clinics, uh, that we're gonna go dive into a little bit deeper today.
And one of the pillar, as Jeremy mentioned, was about the, the patient experience and automating that, that entire experience and never losing a patient. So going through exactly how to make sure that you are focused on that. That end-to-end patient experience and automating the entire process. Um, another pillar was about people and culture and understanding burnout and retention.
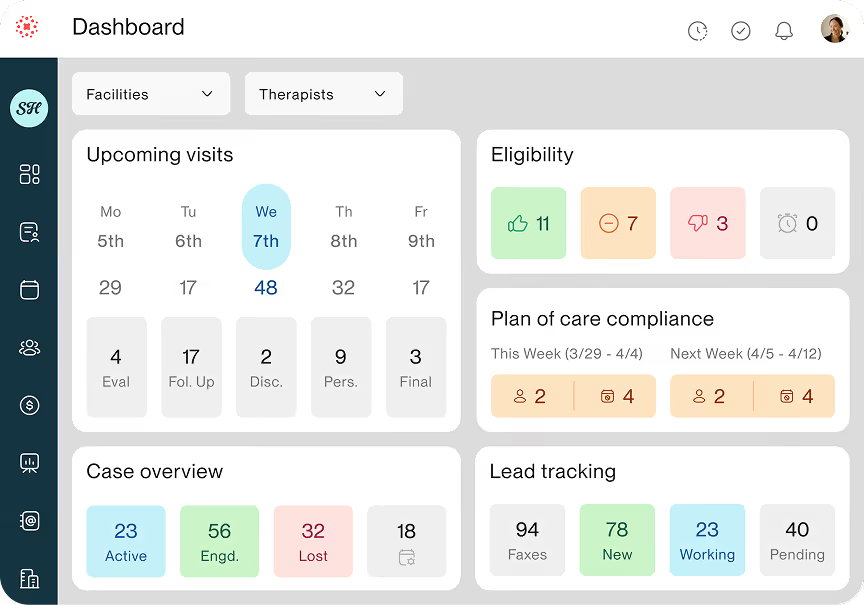
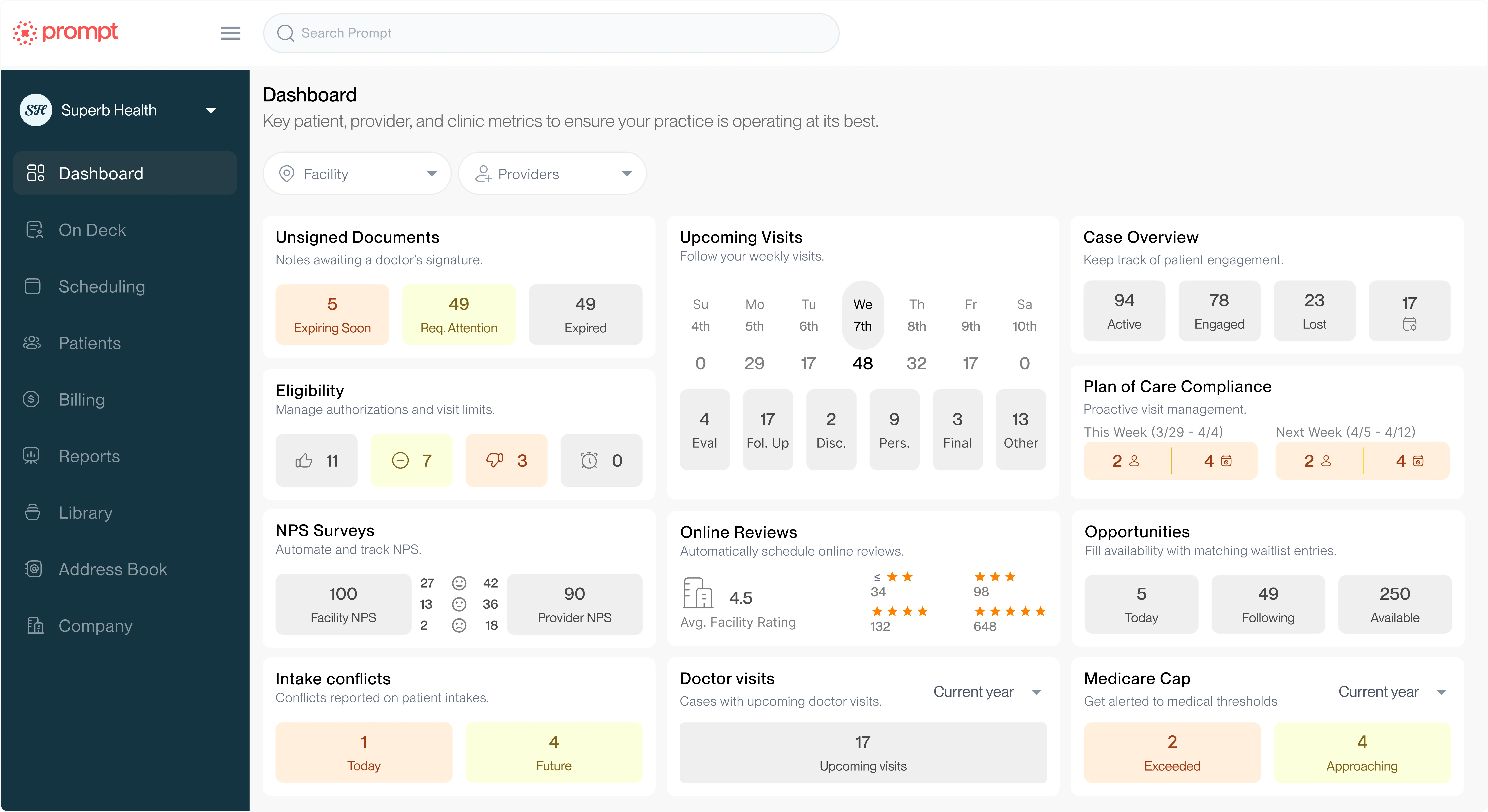
Um, and the third pillar was actually about revenue, uh, revenue cycle management and cash flow and automating that process. So we're gonna dive into that a little bit today, starting with that patient journey. Um, some key data that we saw was 96% of high growth clinics actually used automated reminders.
Um, and that wasn't just patient reminders, it was online scheduling, all of the above. Um, and so intake, scheduling, wait list, billing accuracy, there was about 1.5 x more likely to use digital wait lists in high growth clinics. Uh, 90% of super growth clinics track capacity and productivity. Two thirds use AI for documentation, and we saw high growth clinics were actually two times more likely to use AI for admin workflows.
And that, that sounds pretty similar to what you guys said in terms of automating, removing some of the processes. Um, so Jeremy Love to ask you, where do you think clinics fall short in that patient journey and how costly are cancellations and no-show to growth?
Jeremy: Yeah. Um, I could probably give an hour talk on this.
Um, it's so important to me that, uh, we actually brought, um, someone who's a leader on this front into our, um, on our team at Quis, uh, Jerry Durham, who lives his life, breeze his life around the patient, experience the patient journey. And I had met with him, you know, a year ago and I was just astounded by the simplicity of that.
Um, but also the impact, and it's not just physical therapy. This is across all healthcare services. I think it's a. Um, it's a matter of, uh, just challenge when you're balancing reimbursement and, um, cost and, you know, flow and all of this. And fortunately today, automation creates a great opportunity to, to do this much more efficiently than, you know, in my generation when you had to do, know, write the stuff on, um, you know, cards and notes.
But, you know, to me, the, uh, at the end of the day, I, I always come back to the fact that, um, a, a cancellation, a no-show, at least that I, when I was treating patients, I, I took it as a personal front. Um, I challenged myself every time I had a simply a cancellation or no-show. I was, what did I do wrong? I, I failed the patient.
Um, probably a little bit, um, overly hard on myself there. But the reality is that I think every single patient that comes through your door, they're looking for something. And it's that connectivity to the therapist. It's that it goes beyond just the intervention you provide. It's, it's listening, it's learning, it's understanding of them.
It's putting an arm around them. And it's, it's really being a, uh, human to human connection that goes far beyond the, uh, clinical intervention. And, you know, Marla, we worked together and known each other forever and you taught me the term therapeutic alliance, and it's something that's been embedded in my mind.
And, you know, we also had an opportunity, some really cool research on this and define what are the drivers of patients falling off the calendar or off the schedule. And you know, what we actually found, um, in our research together was, uh, largely it's driven by the type of intervention they or receive and the coaching they get on visit one.
And, you know, a lot of times therapists, they'll, they'll do what I think is a overly complex and complicated evaluation and they lose track of the fact that patients are coming through their door, generally speaking, to feel better that day, that moment. Um, there's other professions who a wonderful job of this and they're saying, you know, um, you know, chiros are an example.
They do a great job of. You came in here for back pain, I'm gonna treat that and make you feel better, and then we'll work more progressively down the line to get you better. But I wanna make you feel better. And, um, we can't lose track of how important it's on that first, second, third visit with a patient to build their trust, make them feel better, put our hands on them and show them delay and coach them.
'cause what we found is that the, the fall off a patient's e occurs generally and visit one through three or visit six plus visit one through three. Is that initial connection point you just didn't, didn't make it work for them and they found something else. Visit six plus generally is we as therapists ran out of either steam or creativity or, uh, aren't evolving our treatment plans to meet where they need to be, and they simply just sort of float away.
Um, both of them are, are massive failures both to ourselves and our clinics, but even more importantly in the, the overall profession, you know, what's the cost of a, of a patient? No-show to me it's, I don't know if you can calculate that. I mean, you could simply say a case is worth a thousand bucks and say I lost a thousand bucks, but I don't think that's it.
I think that in a universe where only 10% of patients who need our services actually make it through our doors, this is an opportunity to build the brand and to build the identity of physical therapy for the overall patient community. So when a patient no-shows and uh, checks out of our care plan, I think that that's probably a 20 fold loss because generally speaking, people tell the story of, uh, things that weren't good, much more than they tell the story of things that were good.
People always will tell you, I got sick at this restaurant, or the food was terrible. They're not as inclined to say, oh my God, it's the best food I ever have. It's sort of an ex expectation and we need to make the expectation to be exceptional, great care every single time and not let patients fall off.
So I think that you magnitude this, it's, it's an enormous impact that is really in our hands, and we can control this just by that therapeutic alliance that addressing the patient need immediately wrapping our arms around them and building goals with them that they totally understand are on board with.
Marla: Absolutely. And, and like you said, it's invaluable. It's not that a thousand dollars, it's well beyond that 'cause they're talking to others. Um, so with that, Ken, I know your clinic does a really good job about using technology to automate that process of the patient journey and experience. So love to hear what changes did you make that had the biggest impact on the cancellation and, and scheduling and making sure that patients didn't fall off.
Ken: Yeah, for sure. So, um, you know, there's the easy stuff, right? So automating on the front end at that initial experience where somebody can come in, you know, they can schedule online, they can go through that process. Automating on the authorization and verification process, utilizing the clearinghouses using, um, like p verify, you know, switching over to prompt, shameless plug there.
So, um, just some of the automation that prompt enables, uh, just at that initial experience. Um, the biggest thing, Marla, to kind of echo what, what Jeremy was saying, if, if a patient's bought in to what you're doing, they're gonna be more inclined to, to, to stay, to want to complete that plan of care, to want to come in.
So the other things that we've tried, tried to take advantage of is automating the clinician experience. Um, because the more we can help them with either AI scribes, the more we can help them with AI documentation to remove the minutiae, remove the little parts, the more they can spend more time building that connection with the patient, making sure the patient kind of understands how important they are to that therapist.
Um, because now the therapist isn't bogged down by, you know, stuff, right? They're not bogged down just with having to make sure that, you know, the, uh, the, the node is completed the right way for United Healthcare. So, um, making sure that automation isn't just thought of as tech, making sure that maybe it's systems and processes, maybe it's handbooks, maybe it's whatever you can do to empower the autonomy of the clinical and front end staff so they can solve problems themselves.
So there isn't a barrier. So there isn't just a negative experience that might trickle down to the patient. Then on the back end, trying to make sure that, you know, that last point of contact with the patient, if there's a patient statement or a balance, and making sure that is handled as efficiently, as quickly and accurately as possible.
And then also drip campaigns. Also trying to make sure that patients, once they're a part of our, um, family, once they're a part of our culture, that they know they're not just forgotten about. It's not just you're discharged, go on, do your thing. Um, so we also automate with our clinicians. We want them to follow up with the patient just to do a check-in visit, not to bring them back in, not to kind of, Hey, get back in for pt, but really, hey, here's who you discharged a couple of months ago.
You know, why don't you reach out in a phone call, but why don't you reach out in an email, just check in, ask how their dog is, how their grandkid is, some kind of connection that you recall from your visits. Um, because again, those are the people, like Jeremy was saying, they're gonna tell people the food there was wonderful.
You know, they're gonna tell people that care was exceptional. That's where you gotta go for therapy.
Marla: Yeah. Yeah. And honestly, like you said, it's, it's not just automating the, the patient, but it's the provider experience and making it so easy for that patient to click a button and get in to, um, be able to see how many visits they have on their, on their plan of care compliance.
And also to be on a wait list so if something opens up, they can get right in. And then your clinicians actually have that. Full experience as well so they can focus on the patient. That, that's fantastic. Um, and Josh would love to ask you a little bit, because we saw in the survey that, uh, high growth clinics had all connected systems versus bolted on.
A lot of times you try to get this product, that product and another product. But what happens when all these bolts on and disconnected tools? Uh, what tends to break first or what happens when systems aren't integrated in order to try to scale and be a high growth clinic?
Josh: I think a lot of, a lot of the times it, it, it creates, you know, operational blind spots.
Um, it's not very efficient at all. Uh, data accuracy is a big one. You know, you could have double entries or mismatched records. And again, that goes back to what I first said is like, now you're paying somebody to go track down the correct data or clean the data up. Um, and then, you know, if the patient is getting mixed messages from these systems, that's not a great experience either, right?
So there goes revenue out the door because you're paying someone to do something that they shouldn't have to do. It's important to do so that those patients don't get mixed messages, right? That they, they're proactive about that, but it's not bringing really any value there. So, um, you know, it, it creates workarounds.
You have to do a lot of workarounds as well. Um, again, not being very efficient at all. And just when you're fully integrated, it's not only about convenience, it's about the control you have, the predictability you have and the accuracy you have. Um, and the more accurate everything is going out to your patients, the more you're getting that message you wanna send.
Right. Which ties back to Jeremy and Kim and that whole patient experience creating the less of those drop offs, uh, less of those no shows, um, less of a message maybe you don't want to be sending when everything's integrated like that.
Marla: Yeah. Yeah. And I would say, you know, automation is, is so great, but it only creates leverage when systems are connected and when you wanna be that high growth group.
You don't want people logging into multiple million different processes and having different operational procedures. Really everything flowing seamlessly is really important.
Josh: That's exactly right. If the clinicians are have to bouncing back between dashboards while they're with the patient, they're not paying attention to the patient as much.
Right. There's not that connection there. Um, so things like ai for instance, if it's integrated right into the system, you're then just looking at the patient, talking with the patient, having that take all the important things, uh, that are needed from that visit. Right. So,
Marla: right. Great. Um, and now moving on to the, the next area, which I believe is a pillar. Um, where, where people, people think they're doing really well. But, um, data tells a little different story and that's really an RCM cash flow and profitability. So what we saw in our survey was that high growth clinics are 1.4 x more likely to automate, um, billing and scheduling.
Their 50% of them use reminders and plan of care tracking to reduce drop offs. Um, denial rates vary widely, but lower denials equals automated billing and compliance. Uh, and then the automation correlates with 10% plus revenue growth. So from that end, Josh, this is really your bread and butter.
So where are the biggest silent leaks in clinic, clinic cash flow today? Um, and how do you coach clinics who wanna be high growth to fix those?
Josh: Yeah, I think, you know, high growth clinics, um, everyone I've been involved with, they really understand that, um, everyone needs to talk so front end clinical to, it's an entire RCM process, right?
And when they don't, that's where those leaks can show up. Um, not understanding, um, things like your contracts and your payers to a, a, a granular level, kind of all the stuff Jeremy was saying. That's, uh, you're getting very much in the weeds, right? Um, outside of patient care. So there's certain things like incomplete plans of care if you're not tracking that right.
The, um, people are dropping off at that third visit, that sixth visit, if you're not tracking, um, why they're dropping off. What you need to, to follow up with. Um, you're losing revenue out the door, uh, to those follow and subsequent visits that you could have been having with them to not only get them better, but get that cash flow in the door, um, delayed or inconsistent collections due to denials and, um, rejections that you may not know about, right?
So if you don't have visibility into some of those things and there's no transparency around those denials, you don't know why they're happening. You may think that you should be getting paid for something, but it's already been written off, um, or, you know, you're never gonna get it. Um, so some of those things that you really just need to be on top of and understand, those are the small revenue weeks that happen, but all of them add up.
Um, high growth clinics kind of, they're always obsessing over conversion, completion and collection daily and weekly, not monthly. So it's not something that you're looking back on and going. How did we do this past month? It's, you know, what do we have coming up? How had, how did we do today? Uh, and where are we at?
You know, so you, you wanna stop reacting to things and start being proactive to those things and looking out where you need to, um, in order to stop and plug those leaks from happening.
Marla: Great. Great. Uh, and Ken, you, you mentioned this a little bit earlier when, when we asked about, um, what high-growth clinics are doing, but what, what have you done in your clinics, uh, that have really changed on the billing and RCM side that helped you see a big uptick in revenue and, uh, cash cashflow?
Ken: Um, so we educate. We're very transparent and honest with our team. So we talk to them about, uh, code reimbursement. We talk to them about code selection. We talk to them about, um, you know, if it's a gray area, hey, this pays better than this. Um, again, we're very open and honest with our team. Um, we don't encourage them or we don't demand that they do everything.
We still allow our team to make whatever decision they need to make, but we make sure that we have those open and honest communications with our therapists and just the impact that their choices on the billing screen can have down the road. Um, the, the, the biggest thing that we have again, and, and, and we're super lucky with this, so, uh, we have a director of operations named Janine and a billing manager named Tammy, and they are freaking incredible.
Um, so those two people, they care just the same way. Like my partner and I care, you know, Tammy tries to bloodhound down every, every penny and just make sure that these insurances. Are doing what they should do. Right? We kind of empowered to created a culture where the billing and RCM team is able to leverage, you know, prompt and some of the, um, auto payments and some of the workflows that it has.
Um, but they know that they're not just trying to collect money for this, you know, multi-billion dollar company. They know they're trying to help us as part of the team win against the insurance companies, you know, and try to get us what we were owed by the insurances. So again, focusing on kind of the clinicians and the parts that they can control.
Automating as much of that busy work and minutiae work as possible, and then getting a team that really cares about it, you know, that's been a game changer for us.
Marla: Yeah. And, and using some of the, the technology that actually pops up and lets, you know, what, what code should be used for that. That exercise, whether it's their ex or their activity, sometimes helps give that reminder, you know, I know Sidekick is doing that now, so it's giving it right, right in there so it can help them know there is a better code for that, uh, and they can choose to use it or not.
Um, Jeremy, what about, love to know a little bit the difference between being profitable on paper and having predictable, scalable cash flow, um, and, and your, your thoughts and feelings on what high high growth clinics are doing in that area.
Jeremy: Okay, thanks. Um, I think. I've thought about this question a lot as you're, um, going through the answers and, um, it's really important because it, uh, I think we get lost sometimes in, um, pursuit of profitability and, you know, of all people who know me on this are like, are you seriously saying that you're, you know, very focused on successful business growth?
So, um, and it's not at all my suggesting that how critically important profitability is to any business to be successful, obviously, but profitability is a byproduct of great operations, great care, great everything in your business and profitability will flow. So, you know, it's a, uh, uh, when you, when you lean first into profitability and that's your number one, uh, target, I, I think it, it creates a huge opportunity for compromise on a number of facets.
It can compromise you from a ethical and, uh, just value-based standpoint, of course. Um, that's one part. It can compromise you from a compliance and regulatory standpoint. But also can really compromise your culture. So yeah, I really think it's critically important for everybody who's in a business, whether you're in a scaled business or your own practice, or you want to someday be in practice to think that profitability is the byproduct of greatness, uh, and execution.
Now, when you think about, to your question around, uh, what's the difference of on on paper profitability versus predictable cash flow? It's kind of the difference between like on paper wealth and what's actually in your bank account. It's great. You've got a, an asset that's worth, you know, a bunch of money, but you can't sell it.
And what's it worth? It's, it's worth the paper it's written on until you can actually sell it. Similar thing here in a practice, it's, it's really all about cash flow. So what I would encourage anybody in private practice or um, any beyond even private practice just to think about is, um, you, you get leverage from cash on your balance sheet and, you know, cash on the balance sheet is, it's a reserve that prepares you for rainy day.
And what would I recommend? I think any business that is. Uh, going to be successful, sustainable, scalable really needs to strive to, to hold six months of operating cash flow on their balance sheet in a cash reserve. That can seem like a lot. I'm not talking about six months of revenue. I'm talking six months of cost.
Uh, it's, it's like what you would be guided to just in personal finance, to have a rainy day fund that you need to have that cash there. We've went all, you know, many of us went through COVID. I mean, uh, could you have a better representation of how quickly things can go astray than, you know, what we went through with COVID five years ago?
But it could be anything. It could be delayed payments from a payer. It could be, you know, you want to shift from in-network to out of network and you need cash reserves. You, all of these things factor into that. Um, and now, you know, how do you get to that being sustainable and scalable? That is all in, in my view.
And, and one of the most critical opportunities in our industry and, and something I've really focused on for over a decade is predictive analytics. We should be able to, um, from the, from the moment that you start a week, and I'll just use a a week as an example, you know, you're, you're only in practice, you're running a, a division, whatever that may be.
And you start the week with X number of patients on the schedule and you've got y number of new patients and you've got z number of slots open. You should be able to relatively tightly predict where you're going to land on a volume standpoint on Monday to Friday. And I've seen this done in practice where, you know, I built models where I could land within less than 1% of, uh, where I started Monday and where I thought I would be based upon understanding the flow of my patients, how many new patients are gonna get scheduled, how's this all gonna cycle through?
And um, I've really been stunned by the number of therapists who. Honestly have no idea how many visits they saw last week, how many visits they are that their budget is. I mean, I did a, a tremendous number of, um, acquisitions and practices over the years and, and leading that, um, in my prior role bought probably 70 companies in total.
And it's astounding to me when I, with sit down and do due diligence with practice owners and they really did not know how many visits they saw last week, how many visits they saw last year, last month, how many patients are on their schedule next week, how many new patients they need to achieve their goals.
This is all about just heads up, dedication to understanding. And there's tons of tools now out there that provide these predictives insights. And I would encourage everybody to lean into those. But first and foremost, you just gotta lift your head up and say. What are my prevailing metrics? Well, it's patient visits are what drives 'em through the door.
And new patients are the underpinning of that, know those numbers and understand that you can project that out and operate your business in a forward looking projected manner using the tools that are there. And that's how you get to long-term sustainable success in your business.
Marla: Yeah, that's, that's great.
Uh, you know, and I, I think a lot of people can, can kind of take away with that and understand and, and look at that today, even leaving their own practices, uh, leaving this webinar for their own practices. And Josh, if you can go in a little bit more to tell me what is that real time data then and KPIs and metrics that you, you coach people to look at, you coach people to really make small changes in so that they can, they can have a better cleaner building.
Um, and how important is that data for making decisions for owners?
Josh: I was gonna say, I want to piggyback off what Jeremy was saying there. 'cause he is absolutely right. Um, when you, you need to be able to project and, you know, with clients, I always say, you should be able to project what you're gonna get month to month with cashflow coming in, whatever your collections are gonna be.
It starts with controlling the variables within what creates that, right? So one is volume, but I also say this a lot is I don't care what volume you see, I care what volume you get paid for. Because if you're seeing a thousand patients in a week and you're only getting paid for 500, you just put your clinic through the admin burden of a thousand patients while you're getting re reimbursed for 500.
Right? And that's not a, that's not a winning, um, equation at all. So. Your denial rate. Um, you should know that if, if it's over 5%, you should certainly start looking into things and what your highest denial rates are. What operational workflows are causing those denials? Where are they coming from? I mean, two thirds of denials within the industry come from upfront.
So right from the get go, we're, we're starting to fail, right? So, and those are really easy ones actually, believe it or not. I mean, one of 'em that's, that's super easy to control is just adding a middle initial because that's what's on the patient's card, but they don't add it to go onto the hifa, right?
Like, that's something super simple. Um, so just looking at those types of metrics, seeing where it is and what, what's like that low hanging fruit, you can, you can just really correct to get that metrics within where it needs to be. Another one, our, our plan of care lengths, right? Industry standards, pretty much 12 visits.
Being able to see that on your dashboard or on your EMR or something that collects that data for you. Trying to get it there and, and then being open, like Ken said, with your clinicians, with your front desk people, Hey, we're not getting what we need to be getting and here's why. And then that goes back to execution like Jeremy was saying, right?
Once you put the why's out there and how you're going to correct it, then you execute. And those are tho, once you start controlling all those variables, once you start controlling all those revenue leaks, I tell clients all the time, if you see X volume, you're gonna land in this window of like one to 10,000 range of.
Of revenue coming in. And that's gonna be monthly. And it's not gonna change unless there's a significant change in a variable. Say a bunch of, uh, clinicians go out on vacation the same for that month, right? And your volume drops, or you add a clinician and your volume raises, okay? So now you're at a different set point, but you should still be falling within this window every month, month after month because all your variable variables are controlled for.
So the more you can do that, the more you can project out and the more stable and less volatile, uh, you know, your revenue's gonna be and your cashflow, right? Because what's good, what is good, uh, uh, for a profit if you're borrowing to pay payroll, 'cause you don't have the cashflow every month, right? Um, so people will say that like, oh yeah, we got denials, but we'll get that on the back end.
Okay, well that doesn't help let you pay payroll this month, right? Like that cashflow need was needed this month. So they're both vitally important for different reasons. Um, but yeah, Jeremy, I mean, hit the nail on the head there and then, you know, the revenue on the back end of that are all those other variables that you have to control.
Marla: Great, great. So profitability is a snapshot. Um, but cashflow is survival and scale. And it sounds like from what all you guys said too is it's also the people you all mentioned about really, um, uh, you know, we heard Ken name his people. It's, it's about the people you can't grow without the right people behind there as well.
So that leads us right into our, our next pillar, which is people, culture, retention, and burnout. Um, and we all know this is a, a huge issue is, is burnout in general. Um, but it's, it's not just a burnout issue, it's actually more of an operational one 'cause it's the systems in place. So, um, what we saw in our data for high growth clinics.
They were two times more likely to automate admin work beyond documentation. Um, two third of them, two thirds of those groups gave raises, um, and, and raised their provider salaries. This year, 50% said burnout was a minute. Each your concern, um, and admin friction directly correlates with burnout. So those are our big takeaways from our survey.
So wanna jump into that and ask Jeremy specifically, where is burnout actually originating from today? Um, and what do you think is going on? Is it documentation, volume, lack of control? Um, but how are we gonna be able to keep and grow our clinicians?
Jeremy: Such an incredibly important question and, and something that is definitely, um, threaded to our industry over the last five years in a, um, in a troubling way.
And, but I think it's in our control, um, as leaders in this industry to, um, to have a huge impact here. And I'm gonna go, uh, a little bit more risky, uh, or maybe, you know, off the, uh, sheet a little bit here with respect to where burnout starts. And I, I, I find burnout to be a, um, lack of alignment of expectations and reality.
Um, and to me that starts in academia, that starts in PT school. And I, I know, you know, we as an industry, we, we as providers, we as leaders have to be deeply threaded into the training grounds for PT students coming out. When you come out of PT school and you think that the world will look like this and reality is like this, there's a big gap.
And then you factor in, you know, um, you know, other burdens that exist around debt, around, you know, salary to debt, uh, ratios. And, and you can see where that burnout comes in. Now, a part of this to me is I, I find some challenge in this where, you know, we have to, um, the, uh, be explicit and I, I think, um, physical therapy programs are really doing a disservice to their students by not having more.
Foundational business education, and even just cultural education as a part of their curriculum. You know, it's a, we can't just rely upon solely clinical skills and then come outta school and say, you'll just learn it on the fly. That's how I learned it was, Hey, you'll learn that when you have a job. And I, I didn't, I had to apply myself to learn all those things, and I had a job, and fortunately I had jobs that allowed me to do that.
But we, I think we need to be in a spot with academia to help push the reality of our industry, which is, you know, there is tremendous opportunity to grow and be professionally successful in physical therapy. How you do that is, in a large part how you as a, as a new therapist, how you apply yourself in your early career.
And, you know, I don't think burnout is driven by volume per se. I don't think burnout is driven by, um, you know, even in some cases, lack of tools. I think it's lack of visibility to a purpose and a future. And the way to address burnout, in my view is to, uh, wrap your arms around your, your emerging therapists, your younger therapists, and show 'em a pathway, you know, uh, be a mentor, um, you know, explore how physical therapist can be so impactful across the entire healthcare ecosystem.
This is not just a job where you come out, you treat patients for 10 years, and you know, that's gonna be necessarily the fulfilling pathway for everybody. There will be some for whom that is a wonderfully fulfilling pathway. I personally love treating patients, but I found a direction in my career that required me to do more, to have my biggest impact, and I had the opportunity to spread my wings and do things that I never really would've imagined I'd done.
Now, another side of that is I was willing to take tremendous risk and be very uncomfortable to get to that place. I, I did things very early in my career that were, um, uh. Hour wise commitments that I, I still look back and I'm baffled that I did 70, 80 hour weeks when I was, you know, 25 years old and, you know, that built the foundation.
And I, you know, I traveled tremendously. I, I sacrificed in ways that, you know, really were foundational to get to this place. But I did that because I saw a purpose and I saw where I wanted to go and I wanted to be meaningful and I wanted to be relevant in this career. And that was a decision I made. So, you know, for, for me, with burnout, it, you know, we, we have to have the tools in place that make the job easier.
Nobody likes documenting. It's not fun. There are millions of opportunities now to do that with a high level of efficiency. No one likes prior auth. No one likes to deal with insurance companies. It's always been that way. That's a painful part of what we do, but we have to find purpose. And I think we also have to, as an industry draw back on remembering how truly important what we do actually is.
You know, musculoskeletal care in this country is profoundly expensive and debilitating to the healthcare system. Like 50% of costs are in MSK care. We as PTs are the tip of the spear to address that, and that's truly like wonderful work that is generation lifting work that we can do. So if you're, if you're focused on like a true bigger purpose of what it is that physical therapists can do and accomplish, I think that starts the ball rolling.
But we need to be in, in organizations and in, um, uh, situations around our peers where somebody is helping you, somebody's putting their arm around you, somebody's guiding you and showing you the bigger direction. And what I've found consistently is it's, it's not one, uh, pathway there. For some, it's clinical education.
They want to be a great clinician and we should celebrate that. We should not, we should not force clinicians to. Leave clinical care. In order to elevate themselves professionally, we need to have pathways for them that they can excel in their craft and be rewarded for that. On the other end of that, we also need to be investing in people who want upside growth outside of being a clinician.
They wanna be a leader, they wanna be an executive, they wanna open their own practice, they wanna do a service line. We've gotta pour into that. And I think it starts with mentorship. It's collaboration, it's support, and it's an understanding that, you know, you've got to build a view of the future that's exciting and fun.
Um, you know, we are inspired by where we look towards, um, you know, I'm gonna end this with a, uh, uh, a drawback. So for everyone, I went to Indiana University and I am a happy person this week because our football team is now awesome. Um, and I got to celebrate that as a, as an alum and to see this process.
But remembering that we were the worst football program in the history of college football a, a month ago. Um, and now we're not. And the reason why. I draw upon that is that Kurt ti, who I think will become down as an iconic coach, um, and someone everybody can look towards, he set a vision, he set a vision of purpose to this program when he came in and said, we're gonna win, we're gonna win with intentionality, with culture, with people, and we're gonna do it the right way.
And from the moment he got there, he did that. I think for us, like that is about, that's how you drive, that's how you prevent burnout, purpose, alignment, focus pathway, bring people around, something they can celebrate and feel great about. And that's how you win. And I just wanted to give an IU reference because you know, it's IU week.
Marla: Yeah. Yeah, I mean, you nailed it, Jeremy. I mean, it really is organizational, it's starting from the top. It's really being connected, clear, and communication with your mission, your values. And Ken, I know this is something passionate, you're passionate about as well. So, um, love to hear how, how you've done that and how you've really looked at the culture in your clinic, uh, and, and how high growth groups are doing that to, to be able to retain and, and grow new clinicians into their, into their ecosystems.
Ken: Yeah, so pretty sure Jeremy must have been in all of our management meetings with 3D because, um, that that's it, right? That that's all there is to it. So. Um, the biggest thing that, that I think is having empathy towards, especially the new grads coming out, because I 100% agree, I think they're set up for maybe not the most success with the collegiate experience, right?
Whether it's debt, whether it's expectation, whatever it is. Um, you know, so I've seen some practice owners who, uh, you know, like a, like an old person in a rocking chair shaking their fist like, well, I did it for half as much and double the work, so you should too. And, and I think times are just different now, right?
I think we need to have empathy with these new clinicians coming out that the world is different. So again, what Jeremy said, putting your arm around them, like again, as as if you want to be a high growth clinic, you need people, right? You need patients to come in and you need staff and therapists to be able to treat these patients because as owners, we can't do it all ourselves.
Um, so mentorship is a huge component of that, that I think the, the new grads coming out and especially like clinicians. They want to know that as owners, we have their back. Um, that even if we are an in-network insurance practice and you know, this clinic down the street is outta network and, and their compensation structure is different, ultimately they need to know that here's our purpose, here's our why.
And a big Simon Sinek guy. So, you know, making sure that that culture and that why is very clear so the person's able to, um, sign on with that. Make sure mentorship is gospel. So our, our clinicians, they treat 38 and a half hours a week instead of 40. Um, so we block an hour and a half each week for either one-on-one mentoring or within the clinic with a group.
Um, because we believe that is like first and foremost. And, you know, mentoring isn't just how to stretch out a shoulder. Mentoring is also trying to learn the person's goals, the person's mission, their why, and as a clinic, as a business, can we help them achieve their goals? Um, so again, the, the thing that we've developed at, at 3D or about to develop is that clinical pathway, right?
So, um, we have 16 locations in, in Jersey, PA and, and soon to be Delaware. Every one of our, um, offices has a clinician who's an owner of that office. Um, so we offer partnership as kind of that pathway, um, but partnership's not for everybody, right? So, um, making sure that if you're offering those pathways and those opportunities that you're not necessarily saying being a clinician's better than an owner or being an owner is better than a clinic director or clinic director, better than somebody who wants to roll out like a golf performance wing of, of a business.
So, you know, making sure that you're able to individualize those pathways as much as possible. 'cause I, I think ultimately preventing burnout I I is tough, right? Like everybody's different, everybody's unique, but the more intentional we can be with outlining the mission that we're on, sticking with that consistent messaging, people are gonna sign up for that and want to be a part of this as long as we're able to keep living up to that and working hard for them.
Marla: Yeah. That's, that's a great, I mean, all extremely helpful points in terms of what you're doing and implementing and it's, it's hard to think of, well, I have to, I have to spend on that. Uh, Jeremy, I remember that being a, a big conversation when, when we were in our working together is how much do you spend on that and what is the, the takeaway from it?
Um, and it's always a balance, but really, it's almost like people, clinicians first, patients second, right? Like it's, you've gotta spend that and would, would love to know Jeremy, what you think that that spend is towards it. That will give you the ROI back,
Jeremy: you know? Um, it, it's such an important thing and I it's a spot you, there's a part of this that's money, of course.
Um, I think clinical education is. Cr so important and it's, it can't be passive clinical education. Here's a Med Bridge subscription. Nothing against a, you know, a vendor, nothing like that. I just said, it can't be that passive. You do this on your own and we never talk about it. I, I come from a generation where you got sent to a course, you went hands-on, you came back from that course and you had to show your peers what you did in that course as in service.
And that's how we did it. And like, you couldn't be sleeping through the course 'cause you had to show your peers, like how you were doing joint modes and like, it was this really powerful part of like, you know, we're investing in you, you come back and invest with us. So I think, you know, using clinical education is that real tie that binds is, is very important.
And getting to a, uh, a structure where, you know, you're investing in, in-person education and active training and, but also giving the therapist the power to choose what they want to choose. I really hate getting too rigid where it's like we have a $1,500 allowance and that's it. Like there might be someone on your team who is an absolute rockstar who's gonna go out there and conquer the world in overhead throwing, and you want to give them more, give 'em more share.
Like, don't make this like a flat plane. It's a line item on my p and l and I can only spend $1,500. That's how you lose people. If you have somebody on your team who is an absolute rockstar and you see that, invest in their growth, have a development plan with them side by side, so. I don't want to say there's like a, there shouldn't be a, a fixed line item cost.
It should only be 0.1% of your revenue. I think it's gotta be something that we all lean into and we invest heavily in. And it doesn't just stop with clinical education. I mean, this is also business and leadership. Education. One of the things that have been, honestly for me, most powerfully impactful in my career development was not clinical education.
I did all that stuff. I went to dozens and dozens of courses. What really struck me was I got leadership, education, coaching, real executive coaching. When I was early in my executive career, I was a physical therapist who got to where I was 'cause of hard work and motivation and you know, some ability and hopefully some intellect.
But what allowed me to stay and allowed me to be successful as an executive was not like my sheer brute force. It was understanding how to channel that and having coaching and like real executive development. We need to provide that same sort of, um, uh, service to our therapist if that you don't, this isn't about being an executive.
This is about being a leader. It's about being present. It's about, you know, evolving to a point. And that all comes down to not having scripted, structured sort of, this is what we do, paint the wall black. It is, I want to know your goals and your desires, and we're gonna create a plan for you and we're gonna go on this journey together.
And if you do that, you know, turnover becomes an afterthought. I mean, we went through this, you know, at scale and, you know, getting turnover, sub 15%, sub 20% at scale across thousands of therapists. You do that by investing in pathways and then having leadership at the ground level, pulling them into that pathway.
You should be a resident because. You should go into this educational development opportunity because I believe in you. I see you. And if you do that, I don't think it's about dollars and cents, it's about absolute intentionality that you are going to lead with your wallet as an owner and an executive, and make sure your people can follow because you're giving them the resources to be successful.
Marla: Yep. And we just had a, um, Josh, you know, you, you can relate to this. Yesterday, we just had Jason Collin come in as a guest speaker to our company and talk about the high performing team effect. And that's exactly what you all just said. It's based on clarity. Clarity of exactly what they're expected, the mission.
Um, what, what is I someone hearing some feedback. Um, we have clarity. You
Jeremy: opened up the chat, Marla.
Marla: What?
Jeremy: Go ahead. I think we got opened up. Maybe there's some background feed. But you're, you're good now.
Marla: Got it. Uh, connection, how connected you are to the vision to everybody in the company. Um, and then communication.
How well is communication working and, and Josh, I know if you, you wanna talk on that a little bit? I thought that was really impactful yesterday.
Josh: Yeah. Well, it, it certainly was. Um, you know, the clarity communication, um, all of that is, is vitally important throughout your. And the mission and where you guys are going.
I think, um, I do want to touch on one thing though. Uh, to end this is, is automation and just what it can do for you and, and how you can utilize it in high growth. You know, because these high growth teams, what you definitely do need is margin good margins in order to grow. Um, and there's only really two ways to do that.
One is raise the roof of, of that right? As that's reimbursement and what you're getting in. Um, and you know, we discussed some of those things. That's by controlling the variables, right, that I just discussed that last time. Optimization of coding, as Ken said earlier, it's all coming full circle now, but you can only raise it so high.
That roof only goes so high in so many localities, right? Uh, especially when you're dealing with insurances. Now, if you go cash base, you can do other things with that, but the other way to get that margin is lowering the floor. Okay. And by that I mean automating things that you would otherwise need another person for.
Um, every time you add a revenue producing employee, such as a therapist, you don't then also wanna be adding an admin, which is a non-revenue producing employee alongside them to support that. That's, that's gonna cost per visit, per, uh, clinician a heck of a lot more, right? So when we add automation tools in, it takes away the need for doing something like that.
You can have a better ratio, better margins, and not only does that, it also allows you to start centralizing and specializing with less people such as os, RCM, all of those things. You can centralize those things. Um, as we know, you know, pretty much if you started de novo in this industry. Which is a new clinic, uh, and you're opening that up, it's usually not profitable till you have three clinicians in there, but you don't also want three admin in there.
Ideally you have one admin, you have three clinicians, you have something like a kiosk, you have automated check-ins, you have automated, you know, things happening there, um, that allow you to have that minimal admin. Um, really with, with automation as a sidekick. Supporting those clinicians doing the great care that they do.
Um, so, you know, that's one other thing that I think a lot of high growth teams have in spades is, is that automation process. Um, so that they can have the right people doing the right things instead of the, the redundancies and adding bloated staff to that. Um, while maintaining the patient experience.
While maintaining the clinical experience. Um, and we use that all the time for, for, uh, recruitment tools, right? Like, uh, in my clinics, um, clinicians come in and they see the side, they see sidekick, they see us seamlessly. It works. Um, we, we utilize prompt. So another shameless plug there, but how seamlessly it works.
And that's something that we really do use as a recruitment tool to get them in the door, uh, to help us grow. So, um, that's just one last thing I wanted to touch on there. Um, and how much, you know. That can help not only in margins, but just in this experience all around the clinic side and patient side.
Marla: Yeah, absolutely. And, and that's just gonna make such a difference between being lean and being able to grow and put the money back to your, your, uh, clinicians versus spending it on unnecessary work. Yeah. Um, and you're getting close to the end, so you're gonna see a quick poll pop up. If you would like more information on prompt, um, more information from Jeremy, Ken, or Josh, uh, please feel free to indicate that we do have a couple questions.
I'll try to get to a few if we can. Um, but let's see what we've gotten here. A couple quick ones. Some people are asking if most of our practices are in network or not. So I think Josh, yours is a network. Jerry,
Josh: we're heavily in network. We are a hybrid. We do cash base, but we, we are, we're heavily in network as well.
Marla: Okay. And what about you, Ken?
Ken: Yep. We're all, all in network. Hmm.
Marla: Okay, great. Um, and then we have a question asking about cancellations and no-shows being challenging in mobile practice. Um, so asking about, um, automated wait list, not always being easy. Any ideas or thoughts for mobile practices?
Jeremy: Almost tough, you know, um, I think you, there's only so much you can do around the illness part.
I think I saw that in the question. You're ill. Whatcha gonna do it. That's a, a debilitated patient that, you know, it's not something that is necessarily a reflection on, you know, any care given. That's just the nature of the, the clientele. So, you know, with that environment comes those challenges. I do think that mobile, um, is very much similar to brick and mortar in the sense that it's the patient alliance.
It is the confirmation of the visit, it's the text after the visit. It's just the processes that you do to hyper engage the patient. Um, and I think in a mobile environment like this where you're, you know, if you lose the visit, you're, there's nowhere else to go. You just gotta be hyper attuned to that and really put the systems in place to make sure you can, um, um, auth, not authorize, but um, uh, confirm these patients beforehand and, you know, stay very close to them and motivate them to get better.
Um, but it's harder. There's no question. That's true.
Marla: And I would say too telehealth and RTM potentially could be good utilizes of that. So you can use RTM afterwards. You might not have seen then, but at least kind of continue to check in. Um, Ken, were you gonna say something?
Ken: I was gonna say Jen, the only other thing you could do, because in mobile it's not like you can book two patients at once just in case.
So if you know the person's a frequent counselor, you can always have them like call you day of and see if you have an opening. You know that that's something we do in the clinic with if there are people whose stuff comes up all the time, we just have them call day of if they don't like the wait list feature, um, we just have 'em give a call and we tell them kind of what, what options there are.
Marla: Right. Uh, and we have a great one from Jake. Most useful automated features in prompt besides the plan of care compliance emails and online scheduling.
D um, do you wanna take that one Ken?
Ken: Um, sure. Yeah. So, um. With prompt. The biggest thing that we've seen value in, uh, honestly, is, is the AI automation from intake, um, just to make the, the clinician experience better. So, you know, the patient kind of fills out the intake survey and then automatically the subjective and assessment can pop over, um, into the eval.
Um, the other thing that we're using at some of the clinics and not all is, is sidekick, is the, um, uh, like the voice to text, um, automation and the clinicians who use it, like swear by it. So we're currently doing like AB testing to see, you know, is there documentation being done faster? Are they doing documentation less outside of work?
Is it creating that work life experience? Um, uh, and so far, like the therapists who love it, like, or the therapists who use it, love it.
Marla: And Josh, what about the billing side?
Josh: Yeah, I was just gonna say from the back, the backside of things, the billing side of things, the backend, um, making it more efficient is definitely the auto poster.
If you turn on the auto poster and put in the correct payer rules, uh, for that, it helps tremendously. Um, you know, they can, they can focus on things like calling the payers to talk about those more ambiguous, uh, denials or whatever. And again, they can just be a lot more proactive instead of sitting there posting things that would otherwise get posted anyway and they shouldn't even be having to look at.
So I would say that's one of the biggest game changers for billing teams.
Marla: Perfect. And I'm sure we can go on and list quite a few more, but uh, we are at the, the end one o'clock and you guys all probably have patience. So just wanna say thank you so much for coming today. Thank you to our panelists for all of your great insights.
Uh, growth is really not random. It's deliberate, systematic, and strategic and we hope that this has helped a little bit. Please feel free to reach out to us if you need anything. Uh, we will be sending a recording of this. We will post the link to the survey in the chat and that will go out as well. And, uh, we will be hosting many more of these.
So until then, keep removing friction and improving your systems and we look forward to all of you guys being high growth clinics in the future. Thank you so much.
Lauren: Thanks. Thanks. Thanks guys.
.png)
.png)
